Why we are failing to provide the right support to people and what we can do to fix it.
Author: Tim Keilty
I recently dashed off a flippant tweet demonstrating a timeline of changes since Winterbourne View, a timeline of efforts to Transform Care. Since I wrote this Edenfield has happened. You could probably swap the name of the scandal with any over the last 100 years.
Sadly, we are fooling ourselves if we don’t acknowledge these things are going on all of the time. Massive failures of the system, but also failures in us, our communities, our neighbourhoods. These places exist because we ‘export’ people to them.
What follows is a very simplistic view of what I reckon is wrong, how we got here and one very simplistic idea of what might help.
In the short term this simplistic idea might help some of our brothers and sisters move out of Assessment and Treatment Units more quickly, more sustainably and offer people the chance of a life not just a placement.
Spending time with Simon Duffy has convinced me that there are possibilities beyond this short-term aim, and in the longer term this simplistic solution could also play a part in reshaping social care, even just a little bit. It could also play a small part in helping us, in our neighbourhoods, to stop ‘exporting’ people.
We are, once again, in the middle of sweeping changes which may well solve all of this. Here’s what it looks like as a simplistic cynic:
“Hello Mary! I haven’t seen you in ages… didn’t you work for the PCT?
Yeah, I’m with the CCG now.
I thought they were changing?
Yeah, I’ve got a new job with the ICS…”*
*PCT (Primary Care Trust) CCG (Clinical Commissioning Group) ICS (don’t know)
I’m a bit haunted by my own professional experience of supporting someone to move into his own place a few years ago, things didn’t go as well as planned, I did loads of things wrong which I still beat myself up about. So, when I’m slagging the ‘system’ off below, rest assured I’m slagging myself off as well.
I’m troubled by a brilliant, funny, insightful woman I worked with a couple of years ago to help her escape a local hospital. We snatched time in between lockdowns to plot her escape, she’s still there…
I’m also troubled by a friend and her daughter I said I’d help but couldn’t make the time, then became too embarrassed to apologise.
I know that the last thing these three people need is a new model. Nevertheless, it was these three people who spurred me on to create MY NEW MODEL! There is nothing new in it, somebody else has probably already written about it or is already doing it, so apologies.
In all of the things that I think are wrong I am equally complicit. And for every ‘wrong’ there are brilliant and notable ’rights’.
‘Convenient places for Inconvenient People’ is a phrase from Jan Walmsley which really stuck. People end up in hospitals or other ‘convenient places’ often as a result of a small problem in people’s situations which is ignored. Once ignored, it turns into a little crisis, which is ignored, or families are blamed, then turns into a big crisis. We are so stretched that even a big crisis requires a referral, or an assessment and then it’s a massive one.
At the heart of a lot of the stories I hear from people and families there is a relatively small ask for support which was ignored… or a fight for a diagnosis which was challenged.
Listen to people and respond. I heard a terrifying story on the news that children were being taken into care because their families were too poor to feed and clothe them properly. So, the state will give another family £400 per week to foster the children when a £100 per week would keep a family together. It isn’t always that simple. From my work with Looked After Children (trying to spend money paying for placements, to keep children at or return children home) When we were supporting families to come up with practical and creative solutions parents frequently said, “This is what I was asking for when things broke down, but nobody listened.”
(In no particular order.)
People are supported in hospital in a completely artificial environment which cannot (and should not) be replicated in the real world. There they are treated, or become compliant, or become so cheesed off that they are moved. People escape or are released into a world which is much less restrictive, some people struggle with that. We’ve taught them how to live in hospital, they’ve complied.
We create innovative models (which are sometimes just the old ones with different names) to avoid people having what we would all want for ourselves; a home, a purpose, fun, love, freedom.
People are forced to share with others while in hospital and outside, a lot of people’s anxiety, stress and distress stem from difficulties enduring life with others they haven’t chosen, can’t stand, who wind them up, put them on edge, create stress and distress. When people are stressed, distressed and angry, we add some more paid people into the mix.
People are supported in hospital by relatively highly paid people, in secure environments with huge staff ratios (sometimes adding to their stress) and extra support on hand when things get dicey. These placements cost £4000-£6000 or more per week. When people are discharged it is suddenly OK for that person to be supported by people on the minimum wage.
We have broken people, broken their will, broken their spirit and exhausted families by the fight we make them have. We lose people, forget their identities, ignore their gifts, brilliant, beautiful souls lost from the world - forgotten their humanity.
If you have been in services like these you will very likely have experienced trauma personally – assaulted, raped, physically, emotionally, verbally assaulted. This trauma is often ignored and we struggle to treat people for this (or prosecute the offenders)
And much, much worse.
People are held back by the system and the peculiar fetish of ‘readiness’ People are waiting to be treated, when really we know that treatment will be life-long, difficult and may not even be successful. We make them wait for fun, friends and freedom – things which may knock some of the edges off the trauma.
A brilliant woman I worked alongside recently, was told she could have trauma therapy when she had been ‘self-harm’ free for 6 months. Q: Why do you self-harm? A: As a response to trauma…
Imagine that in the real world:
“Hello, which service do you require?”
“Fire service please”
“Sorry we can’t send anyone until you have been fire-free for 6 months.”
We struggle with a disease I call Placementitis - We are stuck with old and dangerous thinking that some places are OK for ‘those’ people – othering - the thinking of asylums, institutions, but now with more glass, and inspirational quotes dotted around randomly. The placement has broken down let’s try another one, the placement has served 28 days notice…
When people do move out, the local health teams are already overwhelmed, people who are struggling with decades of trauma and institutionalisation are supported by well-meaning and ultimately under paid supporters, when things become tricky, support from specialists, psychology, behaviour support teams is too slow to respond.
Some of the liberating advances like personal budgets are difficult for some people who are stuck, especially if the system has broken the will of people and their families to take control.
In my experience the word specialist adds a justifiable 40% on your weekly placement fee. The specialism really means they employ their own specialists (probably trained by the NHS) and the inflated fee pays for what people should already be able to freely access. I’ve been in ‘specialist autism units’ which were assaults on all of my senses within seconds of being there.
We give (or sell) people to services which are owned by venture capitalists. What is that about!? Other than the obvious answer of money. Smaller community-based organisations (often not for profit) are put off supporting these ‘inconvenient people’ by the way they people are sold - people’s negative reputations are front and centre. Smaller community-based organisations are also put off because commissioners insist on PBS specialists, or in house health teams or evidence of specialism (which is a myth).
The system has never really known what community care is. We don’t routinely help people build relationship filled, connected, contributing lives, we talk the citizenship but don’t do the citizenship. Notable exceptions obviously.
We slag each other off all of the time, commissioners, providers, hospitals, social workers, advocates, consultants – in truth we are all a bit shit. We pretend we are locked in a lightsabre battle between good and evil. And we all think we are Obi Wan Kenobi.
We snatch at whatever comes along and do it, then make the people we support do it. PBS, Life Planning, 3 Conversations, The Keys to Citizenship, Individual Service Funds, The Wigan Deal, The Byker Sandwich, perhaps without really deeply thinking about any of it, examining what it would really take to do any of it properly, or really digging into the usefulness.
Sometimes we are just told to do it by someone else who hasn’t really thought about it either. We are like magpies grabbing shiny things and taking them back to our nests. We are so pleased with our shiny haul that we then haven’t got space in the nest for anything else.
Advocacy is a bit broken – IMCA, IMHA, RPR, Care Act, Instructed, Non-Instructed - titles which have become alienating even to me, who has always felt I came from something called the advocacy movement. It’s been marketised, professionalised, tendered out. Regardless of title, referral route or agency, people need someone to help them speak up, protect and fight for their rights, know them and stick with them.
We have broken social workers and social work, they come and go, are reorganised, restructured, we burn them out, they become agents of the state not agents for change, the state’s representative to people not the people’s representative to the state.
We still think that other people’s behaviour can supported and changed, when we’ve placed people in environments, which for any other citizen, would illicit a justified response of resistance, frustration, stress and anger, for the others the inconvenient people this is inappropriate and challenging. (I think Wolfensberger said that.)
The only people’s behaviour we can be sure of changing is our own (Doreen Kelly said that) but we’ve decided we don’t want to change ours. We are so wedded to our new way that we ignore, or are suspicious of, other possibilities.
We lobby the Government for changes and are disappointed when they don’t deliver. All that happens is they create an action plan, create some new posts, shift some workers around with new titles, create a few more processes (with some new acronyms) then count the beans and report back. The brilliant workers in those posts are quickly squashed, we break their will. Why do we expect Government to Innovate? Like Simon Duffy’s Sausage Horse or fiddling on the deck chairs of the Titanic as it sails towards a burning Rome.
So - a lot of things are wrong, I’ve probably missed a few. Wrong not always, but sometimes. And notable exceptions of brilliance in all of the wrongs I have described. And I am as wrong as anyone.
I drew the original of the picture below on a Saturday afternoon when I’d had a bit of a drink, I took a photo of it and sent it to two friends, at the time I thought there was something in it, and on sober reflection I still think there might be. I’ve shared drafts of this paper with people and they all think there’s something in it. I’ve always loved the mantra ‘one person at a time’ this scales it up, still working one person at a time but bringing people 10 people together…
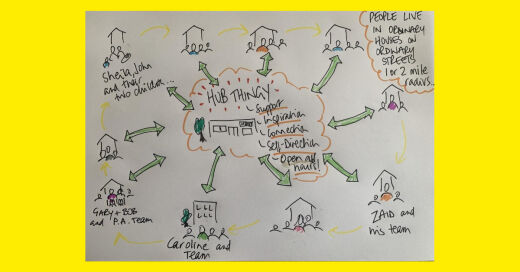
Here’s the basic idea which I think goes some way to tackling what I think is wrong. 10 households - people live their ordinary life in their ordinary street in an ordinary house. Supported by their team, who could be from a provider they have chosen, it might be a family looking after a child with a bit of support, it could be a team of personal assistants, it could be someone who has 4:1 staff. It could be a couple, living with support or a couple of friends. It could be a self-managed team; it could be anything that worked for the person. A one- or two-mile radius would work. Neighbourhood scale.
These 10 households all contribute a 10% (or 15% or 20%) surcharge on their total support costs towards the cost of the support circle/support hub - the name doesn’t matter. Hub-thingy will do.
This could be a Community Interest Company, Co-operative and Community Benefit Society - bottom line it has to be not for profit. It could be based in a community centre, a library, a shop, a house, a campervan, that doesn’t matter either. People supported, families, community on the board, that does matter.
To hold funds on people’s behalf (if they don’t hold it themselves) to keep an eye on how people’s support money is being used to best support them. To encourage creative thinking and creative solutions. These funds can be direct payments, indirect payments, managed accounts, individual service funds – that doesn’t matter either.
To build and maintain circles of support, or community circles to ensure people are not isolated and lost in a little institution in the community – the name of that doesn’t matter.
To create and support Microboards to look after and manage people’s support and budgets if the person has no one else to help or it is too overwhelming to do it alone.
Something like Shared Management at New Prospects (and other places).
The ‘hub-thingy’ builds, creates, supports and celebrates the community it is in, not taking over but supporting existing people/projects and being curious about ‘what needs to be done around here?’
The hub-thingy is well respected, nosey and helpful to and in the community. It pokes its nose gently into things unrelated to Social Care. It supports people involved to contribute their gifts, build relationships, get stuck in.
A bit like Building Community or Fighting for Inclusion? Tim Keilty (see link below), Lives Through Friends etc.
The hub-thingy encourages peer support, it connects people to self-advocacy groups in the area and provides opportunity for the 10 people to get together and support each other (if they want) learning from People Focused Group Doncaster.
The hub-thingy encourages staff teams to connect and share, to support each other beyond their organisational boundaries. Sharing ideas, resources, collaborating not competing. (Paradigm Gr8 support)
Support in a crisis, the hub-thingy employs or has access to people skilled in Low Arousal Approaches (Studio 3, David Pitonyak) or Positive Behaviour Support (lots of people) These workers know the people, can respond quickly (immediately) supporting people through crisis, supporting and mentoring teams/families.
It could provide a place for people’s extra staff, instead of them hovering in people’s kitchens, they could be doing something else productive for the community and drop everything if they were needed.
People will have access to their fund for support quickly to deal with crisis without having to ask permission from a social worker. It could have a friendly psychiatrist on hand. It could have links with nurses Occupational Therapists. Fundamentally it would play a role in inspiring the best possible, questioning, prodding, encouraging - what else could we do?
The hub-thingy does what needs to be done alongside people, fighting people’s corner, ensuring people have access to things they are entitled to, Doctors, Dentists, Benefits, even referring to Statutory Advocacy…a bit like what Help and Connect was intended to be.
I reckon you could make that work, the roles in the team could change… I think for people moving out of hospitals or treatment units the team could consist of:
I can think of places in the North East where you could make this work with existing housing stock. I think you’d find 10 people with really good plans who would want to live in the same neck of the woods. I would work there; it would be lush.
In the short term we could try this with 10 people leaving hospital or an Assessment and Treatment Unit. People so damaged by the system often come with eye wateringly high support costs. I think 10% on top of people’s budgets would cover it If someone is deemed to need 4 to 1 support think in excess of £500,000 per year, a 10% surcharge on that support cost would give you £50,000 - think of it as a membership fee.
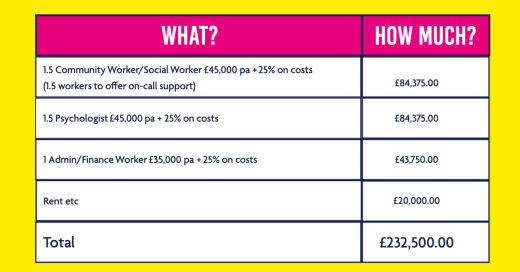
So, 10 people stay out of hospital, get connected, contribute, build peer support, build community for £232,250 per year. You could try it with 10 people for 6 months, you might discover that there’s scope to support 15 people this way or 20 people for the same cost.
You’d need to see people’s support costs to work out a fee - if there was more money than the hub-thingy needed, it could be invested in the community, a Small Sparks fund, a cabin in the woods for people to escape to in crisis, a community carnival…
In the wider social care world, each neighbourhood could have a hub-thingy, serving more people with much smaller levels of ‘needs’ but equal levels of gifts. The personnel of the hub-thingy is fluid and could change accordingly.
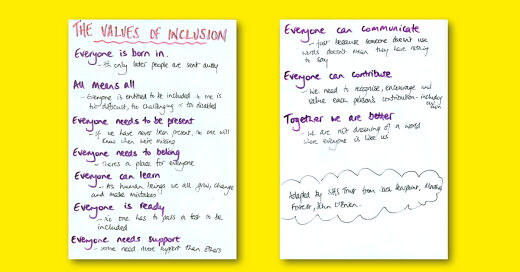
Last but not least – this is the why and some of the how; if it moves away from these it fails:
I know none of this is new, I know it’s got a bit of keyring, a bit of local area coordination, a bit of all of it. But it isn’t core and clusterf*@k.
You could steal this and go and do it – that would be fine (if a little bit cheeky) but as long as you stick to the Rules of the Game go for it, give me a shout if you get stuck.
If you are a big cheese in the NHS you could help us give this a go somewhere quickly.
You could help us refine, build and figure out how it could be improved and how it could have life beyond my first hope of it benefitting the inconvenient people we have exported. Liz Leach Murphy at Imagineer is ahead of the game on that one.
You could help us figure out where this could go in the wider context of Neighbourhood Democracy and Progressive Social Care?
Thanks: I’m grateful to Citizen Network and the Neighbourhood Democracy Movement who are supporting me to turn this Saturday afternoon sketch into something which might, just have ‘something in it’. Thanks to Simon Duffy and Nicola for their generosity, and thanks to everyone who read this and thought there was something in it…
P.S. If nothing comes of this I have an easier suggestion, we should start every professionals' meeting in Health and Social Care, every Conference with the football chant: “We don’t know what we’re doing, we don’t know what we’re doing” that might stop us doing more of it.
The publisher is Citizen Network Research. Building the Right Support...When Everything is Broken © Tim Keilty 2022.
Deinstitutionalisation, disability, health & healthcare, intellectual disabilities, Local Area Coordination, local government, Neighbourhood Care, Peer Support, Person-Centred Planning, Self-Directed Support, social care, England, Article