John Carlisle explains why setting targets for the NHS is both wasteful and diverts attention from the real business of improving quality.
Author: John Carlisle of Mad Management, Sheffield
John Carlisle presented this short paper at the Yorkshire branch of the Socialist Health Association. he explains why targets, which often appear rational and helpful, actually undermine good management in the NHS.
Labour damaged the NHS by its target policy. The Coalition followed Andy Burnham’s proposal to cut the number of targets, but still set them to “name and shame”, which compounded the catastrophic impact of the Lansley bill. In their marketisation drive they have also continued to set ridiculous incentives for GPs and NHS staff, such as the recent £55 for every dementia diagnosis (a Tory pledge). This latter policy just demonstrates the Tories’ utter lack of trust in people, even in our great NHS, and their lies.
Their perception of people is that we are venal and will only respond to selfish incentives, even the most dedicated professionals. It also demonstrates the ignorance among politicians of all stripes of how organisations really work. The following discussion on the use of targets demonstrates this.
The previous Conservative government had set targets in the 1990s – for example, guaranteeing a maximum two-year wait for non-emergency surgery and reducing rates of death from specific diseases. But what was different about Labour's approach to targets in the NHS (and across the public sector more generally) was the volume of targets and the vigour with which they were performance-managed from the centre – via Blair’s Prime Minister’s Delivery Unit (operating according to the principle's of 'deliverology').
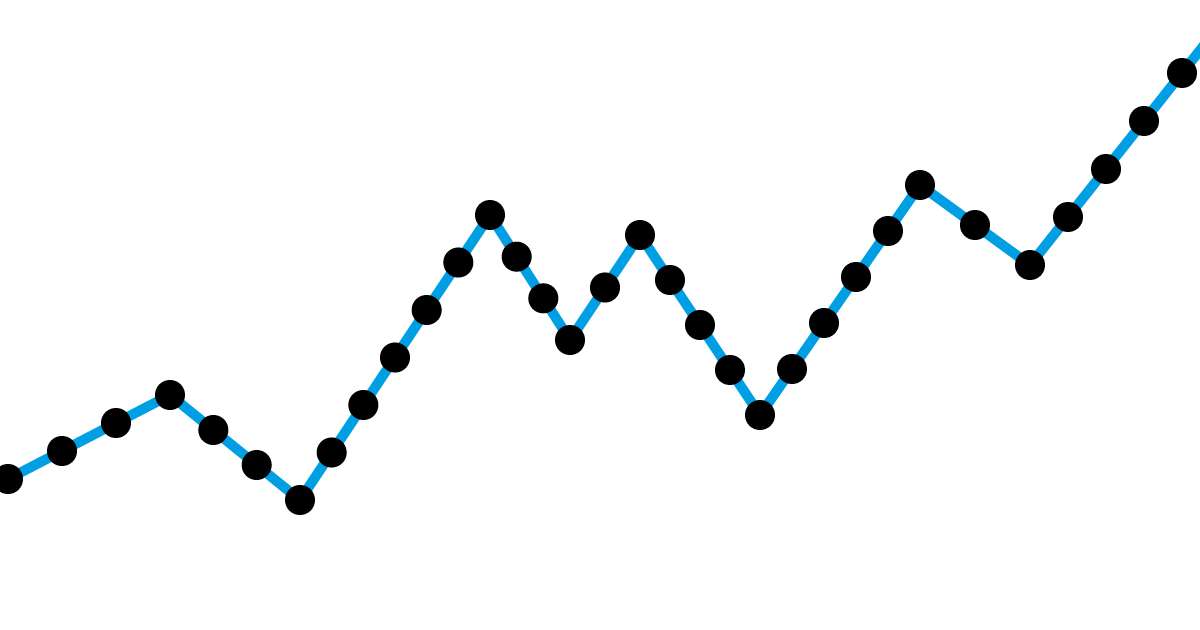
The diagram of targets for A&E diagram below says it all.
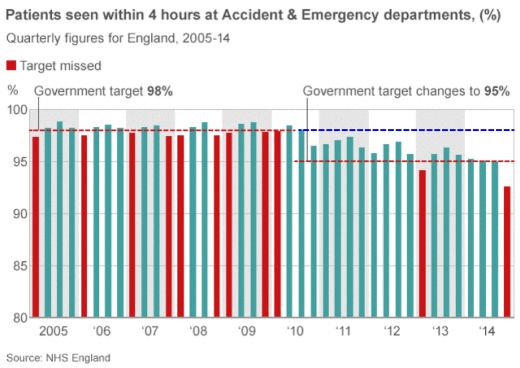
Figure - Targets set without regard to system capability
The Labour government set an impossible target for A&E, treating it as though there would be no seasonal variation. Note, from 2005-2010, the failures occurred in the first quarter of the year, i.e. holidays and winter. What a surprise! But still marked up as a failure. This is mad management, setting up the NHS to fail (98%) 40% of the time. This is equivalent to the battle orders of the Somme ensuring maximum casualties by continuing to drive soldiers en masse into the German guns. Like the generals who perpetrated this infamy, the politicians sit well behind the firing lines, refusing to even look at the carnage caused by their policies.
The diagram says: politicians have designed failure in by their targets.
Having seen the failure to achieve the 98% target the Coalition reset the targets to 95%. This despite the fact that the Tories pledged to scrap targets in 2007, highlighting a series of flaws with present targets, which Lansley himself said "distorted the way the NHS works". (The Guardian, 22 January 2007)
Note that from 2010 to 2015 there would have been a 100% failure rate had the target remained at 98% (the dotted blue line on the diagram). This is the reality. And it would not have been a failure by the NHS staff! Just a stupid policy.
For years the NHS had been punished by targets, for which Labour was largely responsible, especially Alan Milburn, who is now the champion of private health (see below). This was tremendously de-motivating and expensive, as it led to rework, readmissions, and lack of beds; all of which cause the nursing staff great stress and strain and cost millions.
Not only did it cause a drop in morale, but it also caused “gaming”, intelligent professionals subverting the system to survive. Professor John Kay in his book Obliquity quotes the example of an eight-minute response target for ambulances which led to the vast majority of emergency calls getting just that, and almost none recorded as longer. The target changed the way the dispatchers allocated vehicles, presumably trumping the prioritisation of patient need.
To his credit, Andy Burnham, admitted that the target emphasis was a mistake; but insisted that initially it was the right strategy. It never was. It contravenes every quality improvement principle, beginning with understanding the real performance capability of the A&E system. They clearly never understood the principle, otherwise they would never have set the 98% target, understand the variation that occurs, e.g. winter comes every year (note when the targets were missed, above) and, with the help of the staff, transform the performance without causing anomalies. Never set arbitrary targets, and never ever compound the error by using targets to punish or reward people.
Any improvement in results were achieved by understanding and changing the system, driven by the staff. Not by targets! The Royal Bolton Hospital in 2006 is a good example. The staff redesigned the entire process, which improved stabilisation and made access into theatre and discharge rates happen more quickly. The four key effects have been:
But this is ignored by successive governments who insist on the command and control policies led by targets, while ignoring the cries of the NHS employees who were being damaged by the policy, as is evidenced by the fact that between 2001 and 2007 there were about 150 press features criticising, with evidence, the impact of targets. Also in the influential Berwick report in 2014, The Science of Improvement, the word “target” is not mentioned once!
Today, in 2018, the performance levels are even worse: so much for targets! The only other country that set so much store by targets in the workplace was the USSR, and look what happened to their economy!
For more information about John Carlisle and his work check out his Mad Management website.
The publisher is the Centre for Welfare Reform.
Setting Stupid Targets for the NHS © John Carlisle 2018.
All Rights Reserved. No part of this paper may be reproduced in any form without permission from the publisher except for the quotation of brief passages in reviews.
health & healthcare, local government, England, Article